Navicular syndrome in horses: understand, diagnose and treat
Podotrochlear (navicular) syndrome is one of the most common causes of chronic foot lameness. Anatomy, clinical signs, diagnosis and therapeutic management.
Introduction to navicular syndrome
Podotrochlear syndrome — also known as navicular syndrome — is one of the most common causes of chronic foot lameness.
Like any syndrome, it is a condition identifiable by a set of fairly characteristic clinical signs that may have different underlying causes.
Indeed, “podotrochlear syndrome” means a condition affecting the podotrochlear apparatus.
The podotrochlear apparatus is made up of several distinct anatomical structures.
Anatomy of the podotrochlear apparatus
To understand podotrochlear syndrome, you need a basic notion of anatomy.
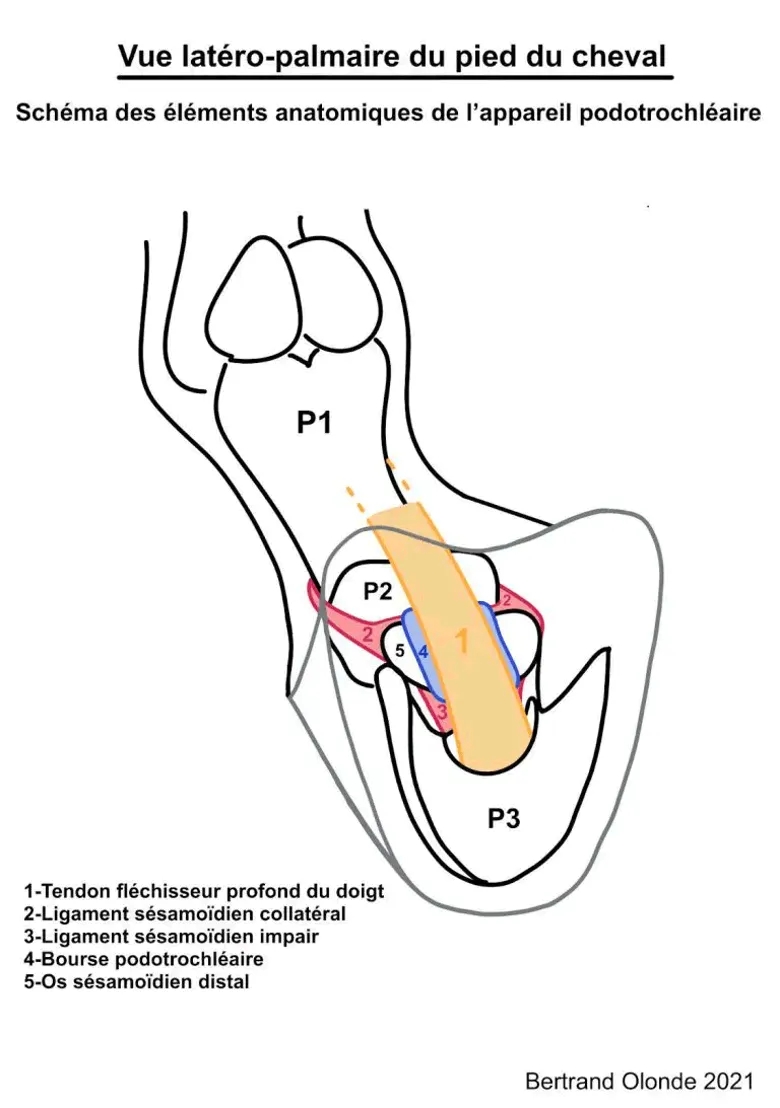
The diagram below (figure 1) shows the main anatomical structures that make up the horse’s podotrochlear apparatus.
The podotrochlear apparatus is made up of:
- 1 bone: the distal sesamoid bone, also known as the navicular bone
- 1 tendon: the deep digital flexor tendon (DDFT)
- Several ligaments: the collateral sesamoidean, the impar, and (to be exhaustive) the chondro-sesamoidean ligaments
- 1 synovial structure: the navicular bursa, which provides a “sliding” interface between the tendon and the navicular bone
Once you understand the anatomy of this region of the foot, it becomes clear that “podotrochlear syndrome” or “navicular syndrome” can hide lesions of very different natures and locations.
This means each case requires its own management plan and prognosis.
In short, there’s “navicular horse” and there’s “navicular horse”.
What does the podotrochlear apparatus do?
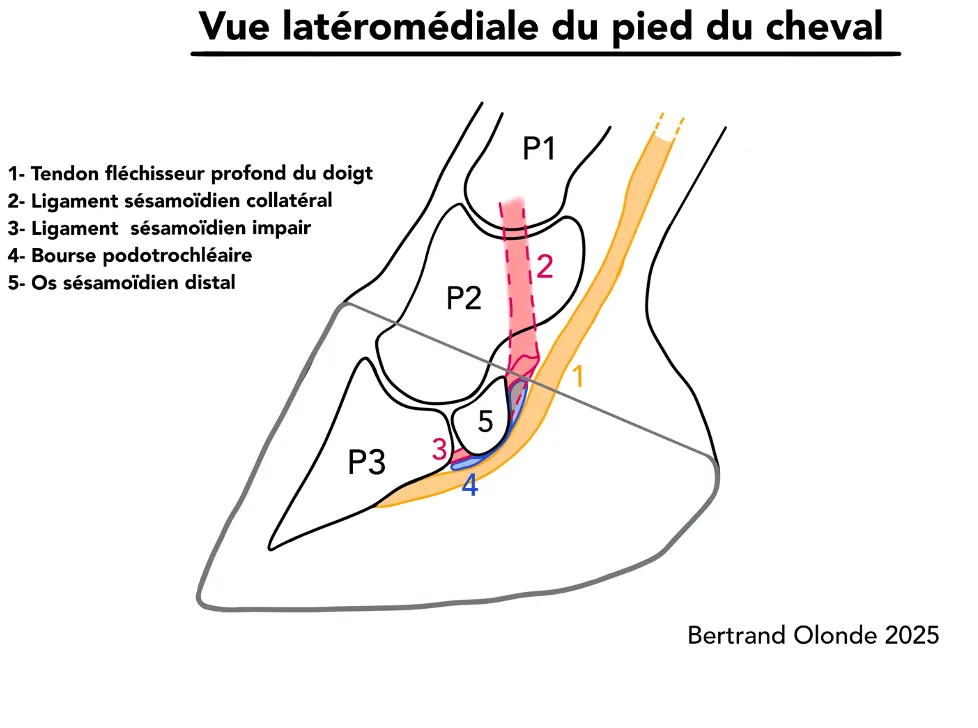
The lateral-medial view (figure 2) clearly shows an inflexion of the deep digital flexor tendon as it wraps around the navicular bone.
The physiological tension of the tendon and its change in direction create pressure of the tendon on the navicular bone.
As a result, during movement, the deep digital flexor tendon must be able to slide on the tendinous face of the navicular bone, also known as the facies flexoria.
The facies flexoria, covered with fibrocartilage, and the navicular bursa — the synovial cavity between the navicular bone and the tendon — are essential to ensure the sliding of the tendon over the distal scutum that the navicular bone represents.

Conversely, during digit extension, these structures come under tension and can cause pain.
Clinical signs of “navicular” conditions
Static exam: visible clues
This is a condition that mainly affects the forefeet.
First, the conformation of the feet and the limb conformation give a number of clues.
Some horses with long feet and crushed heels are more likely to show pain in the back of the foot — and possibly in the podotrochlear apparatus.
Especially if their natural conformation is straight-pastern.
On this point, beware not to confuse a verticalised conformation (compensation) with a naturally straight conformation.
Other observations can be useful, such as the volume of the forefeet (figure 2).
A foot that is significantly larger than the other can reveal weight transfer to one foreleg in particular.
This happens when the pain is chronic.
Next, observing the horse’s postural behaviour is one of the best moments to gather information.
In profile (figure 3), the horse may relieve a foreleg — the “navicular foot” — by placing it in static unipodal protraction (placing the foot forward).
If both feet are affected, the horse alternates this antalgic position from one foot to the other (bipodal pain).
Another postural sign — less visible to the untrained eye — is that the horse may shift its support under the chest to better unload the opposite foot (figure 4).

Also, by the end of a shoeing cycle the heels collapse and the horse’s locomotor capacity degrades.

To complete our static exam, we sometimes observe synovial distension of the foot joint or swelling of the pastern hollow — which is frequent in jumping horses.
Hoof testers or the “plank test” can also give relevant indications about the health of the podotrochlear apparatus.
Note: In the stable, the horse may sometimes position itself with straw piled under its heels to relieve the navicular region and artificially raise its heels for a moment.
Dynamic exam: observing movement
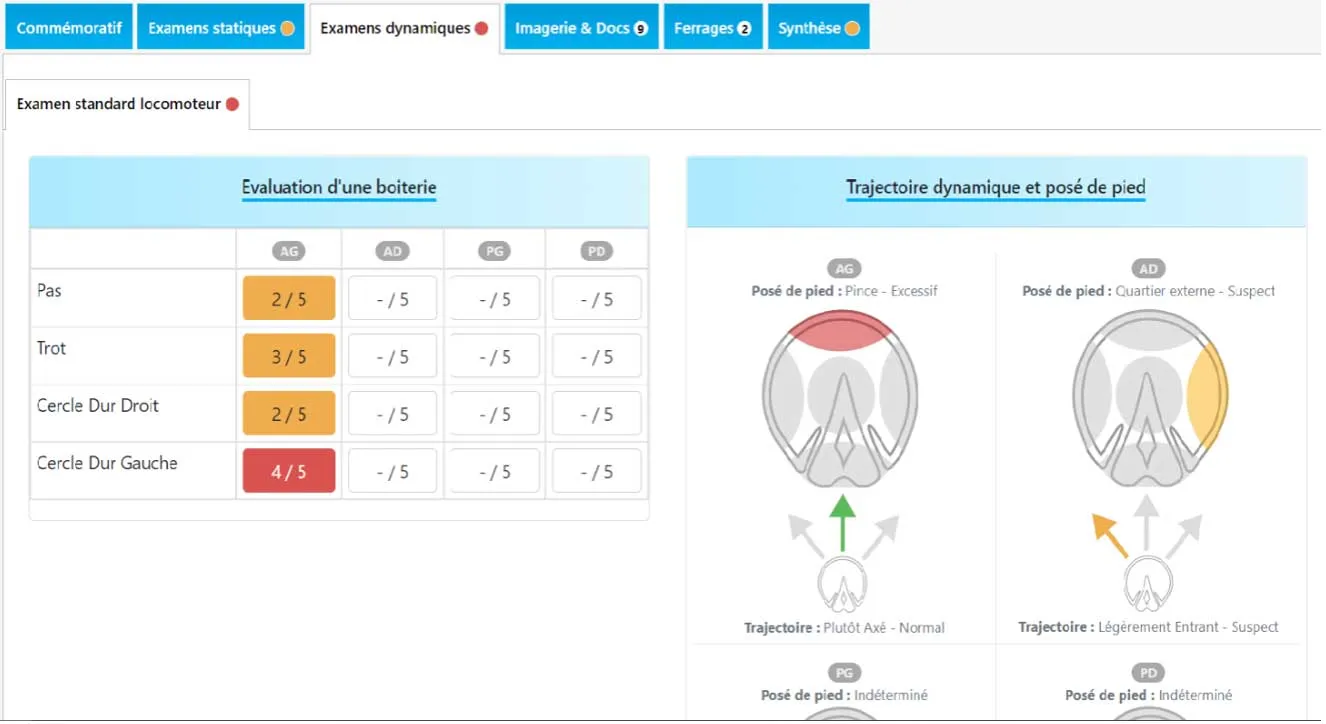
This is the phase of the exam where the practitioner objectifies a lameness and assigns it a grade.
But observing the horse in motion can go further.
A certain way the horse moves can suggest a navicular syndrome more or less strongly.
Indeed, most subjects with navicular syndrome will tend to load the toe of the foot to relieve the back of the foot — the part containing the podotrochlear apparatus.
Concretely, the impact zone of the foot at landing is the toe (figure 5).
We also pay attention to the landing of the sound limb, because the horse can change the impact zone of the non-painful foot and its trajectory.
It’s quite logical: the horse transfers its weight and therefore shifts its centre of gravity towards the sound limb so that movements are less painful.
The “navicular” horse often shows reduced gaits. Certain conditions help the practitioner refine observations.
For example, the lameness may be amplified on hard ground or on the circle. We can also gather information by examining the horse at work or in competition.
In show jumping for example, a “navicular” horse may land preferentially on one foot or lose trajectory.
Diagnosing navicular syndrome
Imaging techniques used
To confirm a diagnosis of navicular disease, you need to rely on imaging techniques.
A radiographic exam is essential as a first step. However, radiography has its limits. It doesn’t allow evaluation of all the foot’s tissues.
We then complement the imaging with ultrasound, or even MRI. MRI is the exam of choice as it gathers the maximum amount of information.
Limits and necessary complements
Modern imaging techniques are very effective at highlighting lesions, but you can’t make a diagnosis from images alone.
Lesion does not always mean pain. Some lesions are well tolerated. Some are degenerative and can appear with age without much consequence either. Others may have impacted locomotion in the past but are no longer active at the time of the exam.
It is therefore important to understand that complementary exams are intended to confirm diagnostic hypotheses whose origin is the clinical exam (observation, palpation, tests, flexions…).
The origin of pain must be determined as precisely as possible by clinical examination, which may include diagnostic nerve blocks. Only after establishing proof of the lameness origin can the radiography or MRI images be properly interpreted.
Managing navicular syndrome
Over the past twenty years, the quality of diagnosis and management has greatly improved.
First, advances in imaging techniques have allowed much more precise lesion description. Then, farriery has evolved enormously to offer adapted orthopaedic shoeings. And, most importantly, prevention has become a focus more recently.
All these factors have changed how a navicular disease diagnosis is approached.
With proper management, a horse with podotrochlear (navicular) syndrome can continue to practise sport — sometimes even at high level.
In the acute phase, rest may be recommended to minimise inflammation, or the horse’s working conditions can be adapted.
Veterinary approach: treatment and follow-up
The veterinarian’s therapeutic arsenal is varied. The first goal is to treat pain and reduce inflammation.
Systemic anti-inflammatories are often used, at least in the acute phase.
Then, depending on the lesion’s nature and the lameness’s evolution, the vet may recommend an injection — or even surgery in some cases.
Long-term management of these cases invariably involves the farrier’s expertise: the orthopaedic approach is always a fundamental pillar of the therapeutic strategy.
The role of therapeutic farriery
This starts with analysing the horse’s anatomical characteristics (its conformation, foot shape, etc.) in relation to the nature of the lesion at the root of the problem.
This analysis — most of the time the result of dialogue between vet and farrier — defines the horse’s biomechanical needs.
Trimming corrects phalangeal angles and finds the horse’s comfort zone within its natural conformation.
For the type of shoeing, we prefer a light shoe with the desired biomechanical effect, while taking into account the horse’s lifestyle and discipline.
In general, the farrier has 3 levels of action to treat podotrochlear syndrome:
- Level 1: onion shoes that protect and limit heel sinking into soft ground.
- Level 2: egg bar shoes are very often suggested for sport horses, but they quickly find their limits in certain uses. Reverse shoes (Napoleon shoes) are also often used during the acute phase.
- Level 3: compensated egg bar shoes, used in more severe chronic cases.
There are still other alternatives, such as the rocking shoe (compensated shoe with a far-back break-over point), effective at reducing tensions on the podotrochlear apparatus, or the H bar shoe that promotes foot break-over.
This “therapeutic” farriery must come with regular veterinary follow-up.
And to make progress possible, the owner must accept follow-up of the shoeings every 5 weeks. After this delay, the foot’s balance is often compromised and the benefits of the shoeing are reduced.
Recommended resources and tools
HIPPOTYPOSE : The collaborative platform for orthopaedic horse follow-up.